CGW4U
World Issues: A Geographic Analysis
Unit 3: Africa
Activity 4: How can location make you sick?
If records have been kept, we can map any disease. Most people don’t think of the geographical nature of disease, but it is a necessary consideration if we want to understand and combat it.
Jared Diamond, in his 1997 Pulitzer Prize winning book Guns, Germs and Steel, sets out to understand the causes of the global inequality. “What we found is that the answer doesn’t have anything to do with people and it has everything to do with people’s environments.” (PBS)
Spatial significance! The unique combination of climate, soils, landforms, vegetation and, of course, people and animals will shed light on why any spot on Earth is the way it is. This is not a particularly new or surprising idea, but Diamond’s book has been used by many to explain different phenomena around the world today.
Let’s look more deeply into how your location can make you sick.
Part A: Location, Location, Location
Notebook
Once again, the answer to the question 'why' comes back to the study of patterns.
- Did MEDCs and LEDCs show the same or similar patterns in the images above?
- What would account for these patterns?
- Is this just as CGP Grey and Jared Diamond hypothesized?
 Issues Café
Issues Café
Looking at the 8 maps each representing the global spread of a different disease, what would account for the patterns that you see?
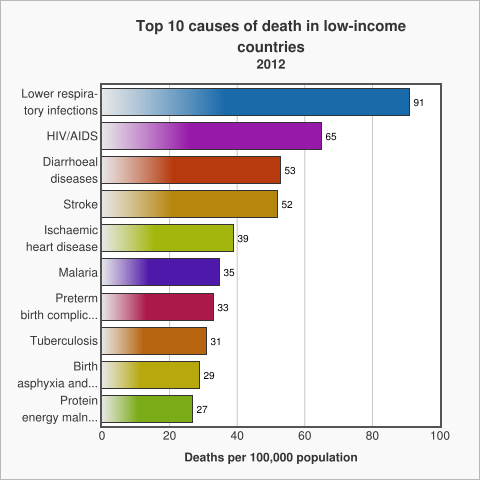
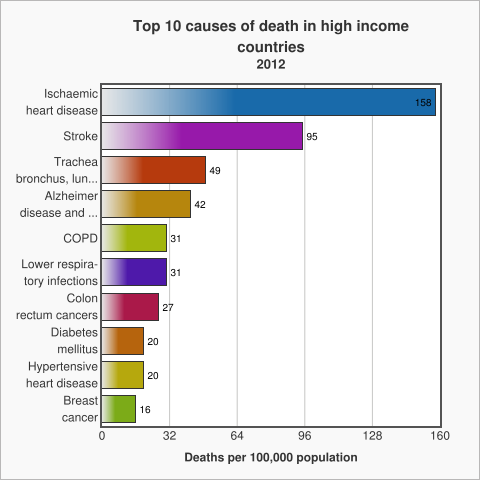
There are diseases that occur in both MEDCs and LEDCs, but according to the World Health Organization (WHO), there are many more differences than similarities. Look carefully at these remarkable graphs. Did you notice that in high income countries most causes of death are chronic conditions/illness? In low income countries, the leading causes of death tend to be infectious diseases of one kind or another. We need to think about why this difference would occur. Is it poverty, location or some other factor that creates this pattern.
World Health Organization
World Health Organization
Let’s look a little more closely at the cholera map. According to the World Health Organization (WHO) today:
- Cholera is an acute diarrhoeal disease that can kill within hours if left untreated.
- Researchers have estimated that there are 1.4 to 4.3 million cases, and 28 000 to 142 000 deaths worldwide due to cholera every year.
- Up to 80% of cases can be successfully treated with oral rehydration salts.
Today, in Canada, diarrhoea is little more than an inconvenience. At the same time in LEDCs it is the third largest killer. The cause is most often cholera.
Has cholera ever been a problem like this in Canada? When Europeans arrived they brought it with them. The first case of cholera in Canada was in 1832. Between then and 1881 over 20 000 people died from this disease. There were 6 outbreaks of the disease between 1832 and 1854 killing another 20 000 of the under 3.5 million residents of Upper and Lower Canada, Nova Scotia, New Brunswick and Prince Edward Island.
Governments in Upper and Lower Canada worked to protect their citizens. In many cases, this meant isolation in cholera hospitals. It wasn’t until there was better understanding of how the disease spread and of the importance of sanitation that outbreaks became less and less common. This is not dissimilar to the experiences of communities in LEDCs today.
The Story of Cholera
It really comes down to health care infrastructure, effectiveness of sanitation and safe supply of water. Without these components bacteria can find places to thrive. Wherever we see these conditions, like in refugee camps, we may also see cholera outbreaks.
As you saw in the cholera map, it is regularly found in Malawi, Mozambique and Tanzania. In regions of countries where modern sanitation infrastructure is not widely available, outbreaks occur with relative frequency. Each of these countries works to improve public education, but often, there is no money to make permanent improvements to water and wastewater infrastructure.
Cholera remains a global threat to public health and a key indicator of lack of social development. The number of cholera cases reported to WHO continues to be high. During 2013, a total of 129,064 cases were notified from 47 countries, including 2,102 deaths. The discrepancy between those figures and the estimated burden of the disease is due to the fact that many cases are not recorded for due to limitations in surveillance systems and fear of trade and travel sanctions.
Today cholera may be considered a disease of poverty. When a country does not have the financial resources to build sanitation and water supply systems, as well as readily available health care infrastructure, problems that are inconveniences for the MEDCs may be death sentences for the poorest people of LEDCs.
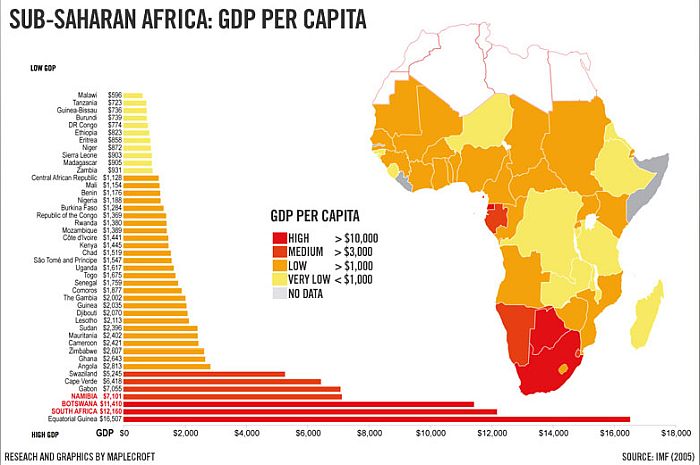
Gross Domestic Product Per Capita in Sub-Saharan Africa
Diamond Facts
Another disease that we don’t associate with Canada is malaria yet it too is part of our medical history. In the 1800s, it was rampant in eastern Ontario along the area that we know today as the Rideau Canal.
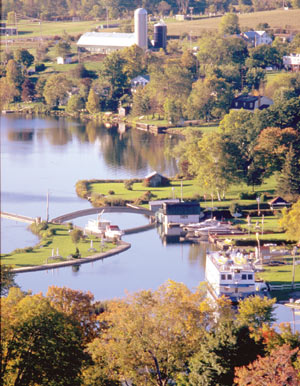
Westport, a small resort town on the Rideau Canal,
where malaria was widespread in the 1830s.
Canada History and Mysteries
Cutting through the swamp and brush between Kingston and Ottawa, the military engineers designing and building the canal were swarmed by mosquitos. Of course, in the 1830s, no one knew that malaria was a infection transmitted by mosquitoes. The thinking at the time was that the ‘’bad air", or "mal aria" was the cause of the seasonal illness.
According to the WHO, malaria:
- Is a life-threatening disease caused by parasites that are transmitted to people through the bites of infected female Anopheles mosquitoes.
- In 2015, 95 countries and territories had ongoing malaria transmission.
- About 3.2 billion people – almost half of the world’s population – are at risk of malaria.
- Malaria is preventable and curable, and increased efforts are dramatically reducing the malaria burden in many places.
- Between 2000 and 2015, malaria incidence among populations at risk (the rate of new cases) fell by 37% globally. In that same period, malaria death rates among populations at risk fell by 60% globally among all age groups, and by 65% among children under 5 years of age.
- Sub-Saharan Africa carries a disproportionately high share of the global malaria burden. In 2015, the region was home to 88% of malaria cases and 90% of malaria deaths. (WHO)
Historically Canada has experienced outbreaks of both malaria and cholera. Cases can still be found occasionally in Canada today, but are usually acquired by returning travellers.
Issues Café: Global Patterns of Cholera and Malaria
Consider the patterns of cholera and malaria globally today.
- Should there be travel bans placed on locations that are experiencing outbreaks of cholera or malaria? If so, who should institute these bans (the affected country or the home country of visitors)?
- Who is at risk when travellers return home and bring with them either of these diseases?
Part B: Is HIV/AIDS about location?
 Question
Question
True or false?
HIV/AIDs is a disease of location.
HIV/AIDS can be controlled and contained.
There are several ways to prevent HIV transmission. (WHO)
AnswerTrue, true and true!
Why then have we not eradicated HIV/AIDS? Why is it so hard to cure HIV/AIDS?
There is so much good news about the place research has brought us to. Hans Rosling, Statistician and Professor of International Health, presents his study of HIV/AIDS with raw data. His concern originates when people make statements like HIV/AIDS is a disease of poverty. Is there data to prove this to be true? If so, all we have to do is decide how we will pay our way out of the situation we find ourselves in. The fact is that this is a much more complicated problem.
Crazy isn’t it? Some places in Africa are more similar (personal wealth and prevalence of HIV/AIDS) to the USA than to other parts of Africa. Yes, there is a very real cost of medical treatment for people with HIV/AIDS. Anti-retroviral treatment means that people can live for decades if they have the money or public health system to cover these costly treatments. But what about reducing or even stopping transmission and the development of any new cases? In the long run isn’t that what will resolve the economic issues associated with HIV/AIDS?
Rosling's argument is that the simplification and generalizations are not respectful nor clever. It can go further than that though, can’t it?
When we build solutions on top of wrong information, or ideas, we can’t get any closer to solving issues. HIV/AIDS isn’t just about poverty. If we act like it is, and send money and the situation doesn’t get better people will rightly conclude that aid (in this case anyway) doesn’t work.
Do you remember the video clip from the first unit about the problems with the Mercator world map projection and why it was so damaging to Africa? This is a similar situation. If we start by thinking about all of Africa as poor, and all the other negative connotations that that suggests, can we ever make positive change?
So, new cases of HIV/AIDS are not a result of poverty, nor war, nor rape. Tanzania and Kenya are proof. Yes, each of these factors plays a role, but there is something more. While researchers work to develop a cure that we know is possible, there is another challenge.
The role that behaviour plays in the transmission of the disease is significant. Some even call HIV/AIDS a “behavioural” disease or a disease that can be solved when we are able to change attitudes and behaviours.
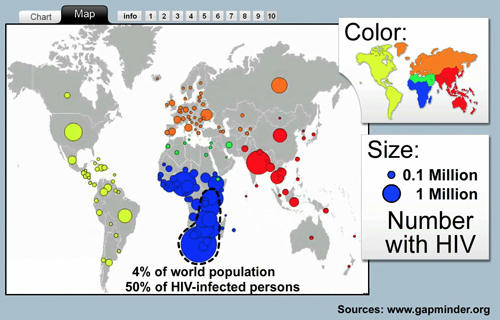
Global Map of AIDS/HIV showing the number of cases and the rate of infection
Gapminder
Before we go on, did you notice the date of that TED Talk? Does that change or alter your thinking about Rosling’s thesis?
HIV/AIDS is not a disease of location; it is on every continent and in almost every country. We understand how it is transmitted. Transmission can be controlled - it is a matter of human behaviour/choice. So we need to ask, “How do different places respond to the same disease?”
This last map shows the number of years lost due to ill-health caused by HIV/AIDS.
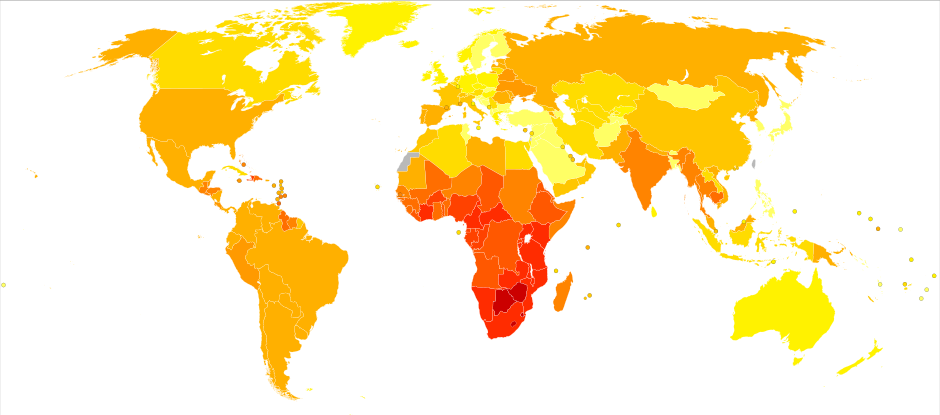
HIV/AIDS is an issue that requires social, economic and political solutions. This map illustrates how heavily it impacts us all. When people are too ill to function, or cannot work because they are caring for an ill spouse or parent or child, all of society interacts with this disease.
According to the UNDP:
Namibia’s relatively small population of 2 million people has one of the highest HIV prevalence rates among pregnant women. Over the last 4 years, HIV prevalence rates within the general population have been estimated to be around 13.5%. Although the prevalence rate among pregnant women dropped from 22% in 2002 to 18.8% in 2010, the social and economic impacts of HIV and AIDS continue to be felt. The HIV and AIDS pandemic continues to pose a challenge due to its dynamic nature in the way it impacts on the Namibian population at large. By 2010, approximately 189,000 people were living with HIV. This number is predicted to increase to 201,000 in 2015/16. In 2010/11, approximately 9,300 people were newly infected with HIV with an estimated number of 25 new infections per day. Of the new infections in 2010, about 40 percent were among young people aged 15-24 and 68 percent of the new infections in this age group were among young women. The spread of HIV is further exacerbated by high unemployment rates, widespread poverty, prevalent sexual practices and high levels of violence against women and children. With about 2 to 3 babies being born HIV positive each day, HIV remains an important cause of infant and child mortality and reaching the virtual elimination target will require sustained efforts in promoting access to prevention commodities, treatment, care and support services.
HIV/AIDS
From the information you have gathered about HIV/AIDS, would you say that there is reason to believe that behaviours, attitudes and research will mean the end of this disease in your lifetime? Share your analysis of the information that led you to your conclusion.
Part C: Is Zika virus a disease of location?
Before 2015, few people had ever heard of the Zika virus. Like malaria this disease is transmitted by mosquitos, in particular the A. aegypti mosquito. Usual symptoms of the virus include mild fever, skin rash, muscle and joint pain, malaise or headache and lasts between 2 and 7 days.The real problem with this virus is that it appears, in some cases, to cause microcephaly.
Microcephaly is a concern for anyone planning to have a family. Zika virus blocks the baby’s proper brain development in utero, or, after birth the head may stop growing properly. These children are born with many developmental challenges and can cost up to $2 million to raise in the first few years of life—though many may not live that long.
 Zika Virus in Ontario
Zika Virus in Ontario
Mosquito bites are common in many many parts of the world. If you live in Ontario you have most likely experienced mosquito bites.
What do you think YOUR odds are of contracting the zika virus? Or having the longer term effect of a child with microcephaly?
What do you think would increase your risk of getting Zika virus.
Research Task - Recife
Based on your study of the above resources, if you could change 1, and only 1 of the following for the people of Recife, which would it be, and why?
- Free and universal access to birth control.
- More mosquito hunters who are in the favela more frequently.
- Increased research on the connections between the zika virus and microcephaly.
Recife
Come to a consensus about which is the change you would make for the people of Recife. Be sure to cite your research.
| Self-assessment checklist for discussion questions: | Check |
|---|---|
| Did I use the question to start my answer? | |
| Did I use facts, terms, definitions or evidence to support my answer/opinion? | |
| Did I answer what is being asked of me such as... Who? What? Where? When? Why? and/or How? |
|
| Does my response communicate the key/important components of the question? | |
| Did I use appropriate written conventions, vocabulary, and terminology from this course? | |
| Did I contribute new information to the discussion? | |
| Have I made connections to the ideas already shared? Ideas discussed in this activity or course? |